If you have a performance mare that you wish to breed without interrupting her career, embryo transfer is a viable option. Palm Beach Equine Clinic (PBEC) in Wellington, FL, offers an extensive range of assisted and advanced reproductive procedures, including embryo transfer. With spring fast approaching, now is the time to plan.
A microscopic view during an embryo flush.
PBEC President Dr. Scott Swerdlin highlights the advantages of the embryo transfer process, which has been utilized since the 1970s. This method is especially beneficial for sport horse mares that cannot afford to take time off for pregnancy. By using embryo transfer, you can continue riding your best mare while simultaneously breeding for your future champions. Additionally, embryo transfer is a viable option for mares with high genetic merit who cannot carry a foal. Some mares may have orthopedic issues that would be exacerbated by the extra weight of pregnancy, while others may have significant reproductive challenges, such as chronic uterine infections or a fibrotic uterus, which hinder their ability to conceive or support a developing pregnancy.
The first step in the embryo transfer process is embryo production. For this article, we are focusing on traditional in vivo embryo production vs in vitro embryo production. In vivo embryo production requires the donor mare to be bred, conceive, and produce an embryo that can then be transferred to a recipient mare. This necessitates the mare being off any hormones like Regumate® (altrenogest) or long-acting progesterone as they suppress the mare’s estrus cycle.
Dr. McNaughten performing artificial insemination.
Strategic breeding management is essential to minimize disruptions to a mare’s training and competition schedule. This may include hormonal manipulation of the mare’s reproductive cycle, a series of reproductive examinations performed using transrectal palpation and ultrasound, a uterine culture and cytology, and breeding the mare by artificial insemination or via natural cover. It is also crucial to document the day and time of ovulation. Whether using fresh, cool-shipped, or frozen-thawed semen, the day and time of ovulation need to be documented to plan for the second and third steps of the process: embryo flush and transfer.
“Knowing the day of ovulation is important,” explained Dr. Swerdlin. “In the mare, fertilization and conception occur in the oviduct, where an embryo will remain for approximately 6 to 6.5 days before migrating to the uterus. Not knowing the day of ovulation might mean that the embryo is still in the oviduct at the time of the uterine flush. Conversely, if the embryo is further along in development, it becomes larger and more fragile, which decreases the chances of a successful outcome.”
To minimize disruptions to the mare’s schedule, most of the process can be performed on-farm, or owners can elect to come to PBEC on an outpatient basis. Veterinarians will closely monitor the mare’s estrus cycle to determine the optimum time for breeding, maximizing the chance of achieving a pregnancy.
“To improve our chance for success, once we determine that the mare is ready, the dominant pre-ovulatory follicle is stimulated to release the oocyte (egg) by administering an ovulatory agent,” stated Dr. Swerdlin. “This ovulatory agent mimics the mare’s naturally occurring hormonal process, and when used appropriately, the majority of mares will ovulate within 24 to 48 hours post-administration.
“Timing the insemination in relation to ovulation is key to success,” he continued. “This is especially true when using frozen semen. For mares that will be inseminated with frozen-thawed semen, we suggest that they arrive at the clinic the same day that the ovulatory agent is administered. This ensures that we can inseminate the mare as close to the point of ovulation as possible.”
The next step is embryo recovery, which is performed 6.5 to 8 days post-ovulation. “The mare will come to the clinic, and the process takes about an hour,” said Dr. Swerdlin. “During this procedure, the donor mare’s uterus is flushed with several liters of embryo flush media. This fluid is recovered and filtered through a special embryo filter to capture the embryo.”
After the embryo is retrieved, it is washed and graded to determine embryo quality. Embryos are graded on a 4-point scale, which 1 indicating excellent quality and 4 indicating a degenerate or dead embryo. Finally, the embryo is prepared for either direct transfer into a recipient mare, shipment to a recipient herd, or frozen for future use.
The final step in the process is the embryo transfer, which requires careful coordination. The success of this procedure is heavily dependent on selecting a suitable recipient mare, taking into account factors such as the mare’s age, size, maternal behavior, synchronization, and overall reproductive health.
“Owners can provide their own recipient mare, but we often recommend that mare owners utilize a leased recipient mare,” noted Dr. Swerdlin. “Numerous recipient herds are located throughout the country, with the closest ones being in the Ocala area. Currently, recipient mares are in very high demand, and each herd has a limited number of contracts available per year. One key advantage of using a recipient herd is that it allows multiple mares to be synchronized to match your individual mare’s ovulation date rather than relying on a single client-owned recipient. For those who prefer to use their own mare, our reproductive specialists at PBEC can manage the synchronization of the recipient mare and perform the embryo transfer.”
The embryo transfer procedure takes place at the clinic. The recipient mare is gently restrained in stocks with the aid of mild sedation. The embryo is carefully loaded into a transfer gun, which is guided trans-cervically into the mare’s uterus. Once the position has been confirmed, the embryo is deposited into the base of the uterine horn. A reproductive ultrasound is performed between three to seven days afterward to assess the uterine environment and confirm that the embryo is developing properly. Recipient herds will often report pregnancies between day seven to nine after transfer.
Frozen semen straws
Dr. Swerdlin noted that the success rate for embryo recovery varies based on the type of semen used and the donor mare. “When using fresh and cool-shipped semen, embryo production rates can reach between 70% and 90%,” he said. “With frozen-thawed semen, the rates are lower, ranging from 50% to 60%. Overall, the success rate of the embryo transfer ranges from 70% to 90%, depending on the quality of both the recipient mare and the embryo.”
Embryo transfer provides an effective and practical solution for sport horse owners and breeders. As the demand for top sport horses increases, it continues to be a valuable tool for those looking to breed that special mare.
For more information on embryo transfer and other reproductive services offered at PBEC, visit www.equineclinic.com or call 561-793-1599.
With modern veterinary technology, there are several ways to breed your treasured mare should she have trouble getting pregnant or carrying a foal. Intracytoplasmic sperm injection, or ICSI, an alternative to traditional embryo transfer is becoming a popular option for the sport horse mare.
According to Dr. Justin McNaughten BVMS, DACT, the equine reproductive specialist at Palm Beach Equine Clinic (PBEC) in Wellington, FL, the ICSI procedure was originally developed to help overcome subfertility in mares and stallions. The first ICSI foal was born in 1996, and since then the procedure has gained popularity amongst breeders for mare and stallion owners alike.
Before ICSI, many breeders’ options for their mare were limited to embryo transfer, which involves breeding the donor mare, flushing the donor mare’s uterus, and then transferring the embryo into a recipient mare that has been synchronized to the donor mare’s cycle. For stallions with limited semen reserves, there wasn’t much that could be done. However, ICSI has become an invaluable tool for preserving sperm from deceased stallions or stallions with limited semen availability as the procedure uses less sperm to fertilize an egg.
A significant advantage of ICSI for sport horse mares, compared to traditional embryo transfer, is that the procedure can be performed at any stage of the estrous cycle, regardless of the natural breeding season. This flexibility allows mares to concentrate on their competition schedules and minimizes disruptions to their training or show commitments.
During the procedure, oocytes, or eggs, are collected from a donor mare’s follicles on the ovary. “It is a valuable option for mares with uterine, oviductal, or cervical disorders that would not allow the mare to be an embryo donor,” said Dr. McNaughten. The ICSI procedure bypasses most of the reproductive tract and goes straight to the source for the oocytes (shown below), the ovary.
Palm Beach Equine Clinic offers the first stage of the procedure, the oocyte aspiration or egg retrieval. Vets will ship the eggs to an ICSI lab to complete the maturation and fertilization processes. During aspiration, mares are sedated and restrained in stocks. The veterinarian passes a long handle ultrasound probe which also houses the aspiration needle into the mare’s vagina. The ovary is stabilized by the veterinarian per rectum to allow for visualization of the ovary and the follicle. The needle is inserted into the follicle; the fluid is aspirated, the wall of the follicle is scraped, then the follicle is flushed and the fluid is aspirated. The scrapping, flushing, and aspirating are repeated multiple times to help dislodge the immature oocyte. The flush fluid that is recovered is then filtered, and any oocytes that are recovered are prepared and transferred into a special holding and shipped off for the next step. The entire process is known as transvaginal oocyte aspiration (TVA) in the US or ovum pick-up (OPU) in other parts of the world.
While the procedure is becoming more routine, it does carry some risks. To safeguard against any risks the procedure is only performed at the clinic. All mares are provided pain relief during the procedure and the following day. “We recommend that mares stay overnight at the clinic to be monitored for any signs of discomfort,” noted Dr. McNaughten, “and most mares return to full work within the week following the procedure.”
Once an ICSI lab receives the egg or eggs, they are put into a maturation media and monitored for 24 hours. “The eggs that we’re taking from the mare are immature, they’re incubated in a specialized maturation media,” said Dr. McNaughten. Each oocyte that matures, is then fertilized with a single sperm cell. “That’s the process of the intracytoplasmic sperm injection or ICSI. If all goes well, the fertilized oocytes are monitored to see if there’s any cellular division or cleavage, which means that fertilization was successful. Those will be monitored for the next 7-10 days until they reach the blastocyst or embryo stage.”
Maturation, fertilization, and embryo production rates can be affected by numerous factors including bred, age, season, level of work, semen quality and whether it is cool shipped or frozen semen. On average 50 to 60% of eggs will mature and be suitable for fertilization. Intracytoplasmic sperm injection laboratories report 70 to 80% of oocytes fertilized typically divide and grow, and 20 to 30% of fertilized oocytes will grow in culture to the blastocyst stage for embryo transfer. The final step in the ICSI process is to transfer the embryo to a recipient mare or freeze it. According to Dr. McNaughten, 60 to 70% of transfers are successful.
In our hands ICSI has become an invaluable tool for in vitro produced embryos not only on the mare side but for select valuable stallions. “To put it into perspective, in a conventional frozen semen breeding dose, the minimum dose is 250 million progressively motile sperm for one breeding. With ICSI, one sperm is used to fertilize one egg,” he explained. “We have also been very successful in producing embryos and foals using frozen semen from a deceased stallions that previously had not produced embryos through conventional breeding management with the same frozen semen.”
Palm Beach Equine Clinic is here to help you achieve your breeding goals. Our veterinarians specialize in breeding and reproduction and utilize the latest technology to ensure a seamless experience for both you and your mare. Contact us today at 561-793-1599 to schedule an appointment or to learn more.
A recent popular post on PBEC’s social media was about retired Davie County, FL, police horse Charlie, who injured himself in true equine fashion – spectacularly and with no one knowing how – during the night while turned out in a field. Charlie was adopted by the mother of one of the Davie County police officers who also works for the Sheriff’s Department. They brought Charlie to PBEC to repair a large laceration on his side.
Dr. Michelle Maguire was on hand to care for Charlie and explained the steps it took to get him back to healing. Dr. Maguire and her team administered intravenous sedation in order to repair with him standing up then injected local anesthesia around the circumference of the laceration, which measured approximately 12 by 18 inches.
“This case was particularly challenging because it was a very large area with multiple flaps and went through many layers, including skin, subcutaneous tissue, and the muscle layers overlying the thorax,” said Dr. Maguire. “Luckily there was no penetration into the thoracic cavity.”
Dr. Maguire used walking sutures to close the laceration, extending from the skin flap’s deep dermis to the underlying fascia of the body wall. This approach helps eliminate
dead space to help prevent seroma formation and infection, reduce skin tension, promote wound closure, and lower the risk of dehiscence, a surgical complication where a wound ruptures along the incision after surgery.
Because the skin can’t handle tension, you can’t just suture the skin itself. Dr. Maguire also used a Jackson Pratt drain, a commonly used surgical drain that provides a constant, low suction to pull fluid from a surgical incision site to decrease swelling and reduce the risk of infection. The drain consists of a thin, rubber tube and a soft, round squeeze bulb, or “grenade” on the end that maintains negative pressure and allows for an active drainage system.
Dr. Maguire noted that Charlie’s prognosis is very good, and he is expected to make a full recovery. He has been doing well at home, and the wound has held together without dehiscence.
She added, “The aftercare protocol was a course of systemic antibiotics and anti-inflammatories, along with maintaining a compressive for the first two weeks postoperatively until skin sutures were removed.
“The horse handled everything very well,” she continued. “He was in pain the first day postoperatively, but as the inflammation subsided, he was a normal happy horse.”
The team at Palm Beach Equine Clinic is happy to report that Charlie is back home grazing. While he will have a scar, it won’t affect his quality of life, and he will have quite a story to tell his friends!
Originally from Corrientes inthe north of Argentina, Lujan Montiel completed her veterinary degree inher home country in 2016, then specialized in treating polo ponies before joining the intern program at Palm Beach Equine Clinic (PBEC).
What is your background with horses?
Over the past eight years, I have worked primarily with polo horses, focusing on their care and management in a field setting — a very different scenario from Wellington and of course from a hospital environment.
When and why did you decide you wanted to become an intern at Palm Beach Equine Clinic?
Since 2023 I have been in contact with PBEC, exploring the possibility of joining the 2024-2025 internship program. My interest in this internship stems from a desire to broaden my expertise and gain a comprehensive view of equine medicine. I aim to specialize further by integrating the intensive care practices performed at the clinic, in addition to learning from the high-level professionals and advanced technology that the hospital offers for both hospitalized and outpatients.
What does the internship program involve?
The program involves rotations through all areas of equine veterinary medicine, including internal medicine, surgery, anesthesia, sport medicine, ophthalmology, and dentistry. The structured rotations, changing every two weeks, provide a unique opportunity to develop skills across multiple disciplines.
What does a typical day look like for you at PBEC?
A typical day at PBEC begins with checking all my patients, performing physical exams, and updating their medical notes. At 8:30 a.m., we have rounds where we discuss cases with the doctors. Occasionally, we have scheduled surgeries, which always start at 9 a.m. Depending on the day and the rotation I’m in, I could be working in surgery, anesthesia, in the hospital, or ambulatory work with one of the clinicians. Therefore, each day can be quite variable and diverse, offering a broad range of experiences.
What aspects of equine medicine interest you most, and what types of cases do you find most rewarding?
The area of veterinary medicine that most interests me is internal medicine. Since my arrival in late June, I have had the privilege of treating a wide variety of cases, including laminitis, colic, neurological patients, diarrheas, and endotoxemia cases, among others.
What is one of the most interesting cases you have worked on?
The cases that I’ve found most interesting and educational have been colic cases due to their variety and the protocol-based management that the clinic employs. There were a series of four colic cases (one next to the other), and all of them were resolved surgically. All of these cases involved a very rare condition called mesocecum entrapment, which prompted significant research into this topic at the clinic.
What’s your favorite part of the job/the biggest thing you have learned?
What I enjoy most about working at PBEC is the willingness of the clinicians to share their expertise in various fields, whether it’s sports medicine, surgery, anesthesia, or internal medicine. Their dedication to teaching ensures that the internship is as rewarding and beneficial as possible, allowing us to truly make the most out of this intensive year of work. Additionally, I have been fortunate to work with a group of interns who have excellent values of camaraderie, making everything lighter and easier when things get busy at the clinic.
When not at PBEC, what do you enjoy doing in your free time?
During my days off, I try to explore the surrounding areas of Wellington, including the beach, as it’s a new country for me, and I love taking the opportunity to enjoy the coastline.
To learn more about the full range of services on offer at Palm Beach Equine Clinic, call 561-793-1599 or visit www.EquineClinic.com.
Fernando J. Marqués, DVM, Diplomate ACVIM, Diplomate ACVSMR
The exceptional athletic abilities of horses can be attributed to several factors, including physiological adaptations, some of which are influenced by training. Muscles, and all cells in the body, require energy to function. Energy from food (carbohydrates, fats, and proteins) is not directly transferred to muscles for biological work. Instead, it is converted into an energy-rich substance known as ATP. The oxidation of carbohydrates, fats, and proteins is the process that produces ATP. There are three main energy systems that supply ATP to the cells: the immediate energy system, the short-term energy system, and the long-term energy system.
The immediate energy system relies on high-energy phosphate sources and plays a crucial role during intense physical activities of short duration that require immediate fuel. These high-energy phosphates are quickly depleted, typically within 20 to 30 seconds of maximum exertion, similar to what happens in humans.
The short-term energy system generates ATP mainly from stored muscle carbohydrates called glycogen. This process does not require oxygen, which is why it is referred to as anaerobic metabolism, leading to lactate accumulation within the muscle cells.
The long-term energy system, or aerobic system, produces ATP during prolonged, intense physical activity. This process requires oxygen, hence the name aerobic metabolism. In this system, fats are a significant fuel source.
The contribution of each energy system and fuel source (carbohydrates, fats, and to a lesser extent proteins) varies depending on factors such as exercise intensity and duration, training status, muscle fiber composition, and oxygen supply to the muscles. Understanding these factors is crucial, as exercise is generally categorized into aerobic/endurance (low intensity over a long duration) and power/strength (high intensity over a short duration). In practice, pure endurance or pure strength activities are rare, and most sports combine elements of both.
Additionally, muscles adapt to specific exercises and sports, which triggers the development of particular muscle fibers that utilize different fuel sources and energy systems to produce ATP.
In equestrian sports, no discipline is exclusively anaerobic or aerobic. Most sports require a combination of both energy systems. For example, racehorses and western performance horses engage in high-intensity, fast-paced activities for short periods, primarily relying on anaerobic metabolism. Conversely, show jumping and polo horses mainly engage in aerobic exercise but switch to anaerobic metabolism to meet the intense energy demands of their sport. Eventing and endurance racing horses, on the other hand, rely predominantly on aerobic metabolism to sustain their energy levels over prolonged periods of activity.
Designing an effective training program for a horse requires considering the optimal adaptation of muscle fiber composition to enhance metabolic function and improve performance in the specific sport.
References:
Hinchcliff K., Geor R., Kaneps A. Equine Exercise Physiology- The Science of Exercise in the Athletic Horse. Saunders
McArdle W., Katch F., Katch V. Exercise Physiology. Wolters Kluwer, 8th Edition.
The warm late summer of 2024 has paved the way for more mosquitos and heralded the start of West Nile Virus (WNV) and Eastern Equine Encephalitis (EEE) season for both horses and humans. WNV and EEE are both equine encephalitis viruses spread by infected mosquitos. They can cause severe brain inflammation and neurological issues in humans and horses and can be fatal in unvaccinated or under-vaccinated equine populations.
With almost daily cases of WNV in horses being reported in several U.S. states throughout August 2024, plus news of humans contracting the rare but extremely serious EEE virus, people are rightfully concerned about how to protect their animals and themselves from both WNV and EEE. The Wellington, Florida-based Palm Beach Equine Center (PBEC)advises on what you can do to minimize the risk of exposure and infection.
WNV and EEE by the Numbers
Both WNV and EEE circulate in the environment between mosquitoes and birds and are spread to horses and humans by the bite of an infected mosquito. However, even though they get sick, humans and horses are dead-end hosts that do not, in turn, spread these viruses back to mosquitoes that bite them.
Since 1999, more than 27,600 U.S. horses have been confirmed to have WNV, with an estimated fatality rate of 30-40%. With yearly activity of around 300 equine cases in the U.S., WNV is now considered endemic, persisting at a consistent level with fairly predictable rates of infection and spread.
EEE, also known as sleeping sickness, causes inflammation of the brain and spinal cord. Mortality can exceed 90% in unvaccinated horses and is lower in horses with partial protection or previous vaccination. Death usually occurs within two to three days of the onset of signs. Horses that survive may have permanent neurologic deficits.
While the diseases sound alarming, the good news is that vaccination is a very effective barrier for your horse. EEE and WNV inoculations are considered core vaccines by the American Association of Equine Practitioners. Annual injections for all horses, preferably in the spring before mosquito season, are strongly recommended. Initial vaccination is followed in four to six weeks with a booster, with yearly revaccination thereafter. Horses living in areas with mosquitos year-round may need EEE vaccinations two or three times a year for full protection.
Clinical Signs
The clinical signs of the two illnesses are almost identical, and can include:
Depression and anorexia without fever when initially infected
Mild low-grade fever in about 25% of affected horses with WVN
Moderate to high fever in horses with EEE
Lack of appetite
Lethargy/drowsiness
Neurologic signs, the onset of which are frequently sudden and progressive
Periods of hyperexcitability, apprehension and/or drowsiness
Fine tremors of the face and neck muscles
Cranial nerve paralysis — facial paralysis and weakness of the tongue are very common
Head tilt, droopy lip, muzzle deviation
Weakness, ataxia, and lack of coordination in one or more limbs
Complete paralysis of one or more limbs
Colic
Inability to stand
Diagnosis and Treatment
A veterinarian will diagnose both WNV and EEE by testing the horse’s serum, a component of whole blood. There is no cure for either virus, but horses showing clinical signs are given supportive care.
Prevention
Aside from vigilant vaccination suitable for the horse’s environment, there are other measures owners can take to prevent infection from both WNV and EEE. They include frequent use of insect repellent, which should be reapplied after rain, keeping horses stabled at night, minimizing standing water, and eliminating areas in which water can collect, such as leaf piles or old tires.
PBEC President Dr. Scott Swerdlin advises, “We can vaccinate against all these diseases, and it’s really important to remember that it’s not just the first set; it takes at least two injections for the horse to develop immunity.”
Swerdlin also points out that horses traveling into an affected region can be put at far greater risk, adding, “People who bring horses to the U.S. from South America or Europe are exposing them to different diseases than they are accustomed to in their native country. They should vaccinate the horses immediately on arrival and then, after the first vaccine, every 12 months. In Florida, where there is a huge mosquito population, we recommend vaccinating against EEE and WNV, as well as rhinovirus, every six months for maximum protection.”
There are no approved human vaccines for WNV or EEE. Personal protective measures include using mosquito repellents, wearing long-sleeved shirts tucked into long pants, and limiting time outdoors from dusk to dawn. Using air conditioning and installing screens further decreases the risk of exposure.
For additional questions, veterinary assistance, or to book your horse’s vaccinations, call Palm Beach Equine Clinic at 561-793-1599.
Wellington, FL – Miss Miami is one of Miami’s longest-serving and most-valued police horses, having joined the team 21 years ago and been through six police chiefs. In the early spring of 2024 at the age of 26, Miami Police Department (PD) had begun to wind down her workload and prepare her for retirement. However, on April 10 Miss Miami looked uncomfortable, and officers called their veterinarian.
“She was not feeling good, and it looked like colic,” explained Lieutenant Redondo of Miami PD. “The vet came and saw she was in distress and said we’d probably have to do surgery. They couldn’t do it and referred us to Palm Beach Equine Clinic [PBEC].”
Miss Miami was driven straight to PBEC in Wellington, FL, where the team carried out a physical exam, blood work, nasogastric intubation, an ultrasound, abdominocentesis, and a rectal exam. Their findings were consistent with a surgical lesion, and she was diagnosed with a strangulating lipoma, a small, benign, fatty tumor that develops within the abdomen and occasionally develops a long, string-like stalk. The lipoma and stalk can wrap around a part of the horse’s digestive system, cutting off the blood supply and resulting in death of that section of intestine.
On the day she arrived at PBEC, Miss Miami was taken to emergency surgery after an initial evaluation and operated on by Dr. Weston Davis DVM, DACVS, who ended up performing a resection and anastomosis, which is where a part of intestine is removed and the two ends are rejoined.
“Miss Miami was routinely induced under general anesthesia; the abdomen was clipped and aseptically prepared for surgery,” explained Davis, who is a native of South Florida and whose father was also a veterinarian. “A midline incision was created, and exploration revealed a large segment of mid-jejunum [the middle part of the small intestine] that appeared to have been strangulated by the stalk of a strangulating lipoma.”
The portion of the small intestine affected was no longer viable, so Davis removed the two-foot long segment of jejunum. Miss Miami’s abdominal incision was then closed with absorbable sutures in the deeper layers and stainless-steel staples in the skin.
Miss Miami was given intravenous fluid therapy including pain relief, electrolytes, anti-inflammatories, antibiotics, and gastroprotectants. She recovered from the anesthesia without incident, and a large abdominal support bandage was applied in recovery.
She was not yet out of the woods, however. Miss Miami’s forelimb digital pulses were mildly elevated in the first 36 hours after the operation. She was managed with digital cryotherapy, and frog supports were applied to both front feet. Her appetite was also diminished following surgery, and she was fed via nasogastric intubation until her appetite began to increase. At that point, her rations were given normally, and the quantity was gradually increased. Her digital pulses returned to normal.
After a week at PBEC, Miss Miami was bright, with a good appetite, passing normal manure, and walking comfortably. She was ready to be released back into the care of Miami PD. Their local veterinarian oversaw the removal of Miss Miami’s stitches a week later, and her belly bandage was reapplied. The Miami PD team was also given four daily exercises by PBEC for Miss Miami to start at home two weeks after surgery to help support her recovery: barrel lifts, butt tucks, stepping backwards, and walking over poles.
“She would have died without the surgery,” stated Redondo. “She has recovered really well. She is still here with us in Miami, but we have started the paperwork to retire her to farmland up in North Florida. Everybody around here knows her and loves her; she’s one of our most famous horses. She’s been here longer than I have, and she’s one of the horses that we liked to use on the regular. Having a horse that already knows the job and is used to all the traffic and loud noises makes it easy, so we are going to miss her.
“The fact that the department agreed to take care of a horse who is old or not being ridden anymore says a lot, and the fact that PBEC took care of her was so great,” he concluded.
PBEC’s kindness and swift action ensured that Miss Miami will now be able to enjoy the retirement she deserves after her years of loyal service. If you or your veterinarian would like to learn more about Palm Beach Equine Clinic and how it can help your horse, call 561-793-1599 or visit www.EquineClinic.com.
As winter winds down and everyone looks ahead to the exciting spring and summer show season, there are preparations that can be taken in your horse’s care to ensure you get off on the right hoof. Close communication with your veterinarian can help you stay on track and ensure everything is properly addressed. Vaccinations, deworming, therapies and treatments, as well as shipping care and paperwork are all important to think about. At Palm Beach Equine Clinic in Wellington, FL, Dr. Elizabeth Barrett works with her clients to stay organized for the upcoming show season.
Dr. Elizabeth Barrett competing in Wellington, FL. Photo by Bridget Ness Photography
Vaccinations
Horses are generally vaccinated twice per year in the fall and spring. If you and your horse are traveling to a new area for the spring and summer season, it is important to think about the requirements of that area or diseases more commonly found there. As an example, Dr. Barrett notes that the Potomac Fever vaccine is not always administered in Florida but can be important for horses traveling to the northeastern part of the country.
Vaccinations also need to be administered with enough time prior to shipping or competing, making scheduling considerations more crucial. Dr. Barrett maintains consistent communication with her clients to find the most optimal day to vaccinate such that it coincides with the horse’s existing schedule. While horse owners and barn managers help organize timing, Dr. Barrett stays prepared on her end by counting her patients and ordering enough vaccines for them.
“The responsibility goes both ways,” said Dr. Barrett. “Usually, the farm manager will let me know that they have some time off from showing, so it’s a good time for spring vaccines. I might also remind them that it’s getting to be time to do that so they can work it into their schedules.”
Dr. Elizabeth Barrett. Photo courtesy of Dr. Elizabeth Barrett
Deworming
Springtime is also a good opportunity to deworm. When horses have traveled from one area to another, it is more crucial. While Dr. Barrett recommends worming twice annually, she explained that it is necessary to pay attention to each individual horse. Examining the horse and knowing the horse’s situation should guide the worming program. Horses that show clinical signs of worms, such as issues with weight and coat, should have a fecal egg count performed no matter what time of year.
Therapies and Treatments
Many horses are completing busy winter show schedules and heading into a break before ramping back up again. This downtime is a great window of opportunity to help address any issues that may have emerged. Dr. Barrett suggests having your horse treated at the beginning of a break to allow more time for the treatment to settle in. Some joint injections and therapies require longer recovery times, so that needs to be planned accordingly.
“After the winter show circuit, I go over all the horses completely to see if there are any issues,” detailed Dr. Barrett. “If there is any lameness or any maintenance we need to do, we try to time it so that the horse has at least a small break before they ship to their next show. Sometimes the horse just needs downtime, and during the spring is often the time they can get that rest. It’s also a good time for different training routines, such as a water treadmill or hill work to change up the program a little bit.”
Shipping
Spring and summer showing and shipping go hand in hand. Remembering all the paperwork that needs to be completed ahead of time is key to avoiding a last-minute scramble. Health certificates and Coggins papers are necessary documents for horses to travel both domestically and internationally. Dr. Barrett notes that it takes at least two days for a vet to complete this paperwork for national travel, so it is essential to keep that in mind when arranging an interstate trip. International travel health certificates take longer to prepare and have more requirements, necessitating additional forethought.
Once the logistics are handled, the horse must be physically prepared to ship. The longer the trip, the more stress it can put on the horse. Even trips as few as three hours can increase health concerns. Stomach ulcers are always a risk, so Dr. Barrett suggests administering preventative omeprazole paste to help keep your horse comfortable. Again, Dr. Barrett stresses that each horse needs to be considered individually, so a horse more prone to ulceration might also benefit from sucralfate when shipping.
“I would scope the stomach of any horse we are worried about that is clinically showing signs that they could have ulcers,” shared Dr. Barrett. “When they ship, it helps to try to feed them a little bit at a time with a steady supply of hay throughout the trip so that their stomach is full.”
Shipping fever and colic are other common issues. Taking your horse’s temperature and monitoring their behavior can help detect the problem sooner. Dr. Barrett also offers a couple of tricks to keep your horse hydrated and feeling comfortable in travel. Feeding a wet mash with mineral oil before the journey helps prevent impaction. Getting your horse accustomed to an electrolyte-flavored water beforehand allows you to produce the same familiar flavor on the road to encourage even the most stubborn drinker.
Additional precautions can be made to prevent other injuries. Considering the horse and weather will guide the best plan. For example, in warmer weather a horse that travels well might do better without wraps, but a horse that is more self-destructive could still need extra protection. Certain halters can cause rubs in warmer weather too. Dr. Barrett cautions that injury can also be caused by a travel buddy.
“It is really important to pay attention to what horses are next to each other,” emphasized Dr. Barrett. “I’ve seen plenty of injuries where one horse is picking on another and causing trouble. I’ve seen more injuries from that than self-inflicted horse wounds, but both can happen. You have to be careful.”
It helps to have cameras on the horses during longer trips to ensure there are no issues. Since the driver usually stops for gas every four hours or so, that is a good time to check on the horses and offer water. For trips of more than 10 hours, it can help to stop and unload the horses to give them a break. Many commercial shippers will drive directly, so in those cases, the health preparations you make are even more significant.
In all of your organization for spring, the most important thing is to stay in contact with your veterinarian. They will be able to inform your decisions, help with timing issues, and make the best possible plan for you and your horse.
The importance of good quality hoof care in competition horses cannot be denied. Farriery can be a major asset during the show season and beyond. The farrier can be proactive in keeping the horse’s feet healthy and thus preventing lameness. Learn more as Dr. Stephen O’Grady of Palm Beach Equine Clinic in Wellington, FL, explains the philosophy behind correct basic farriery in sport horses.
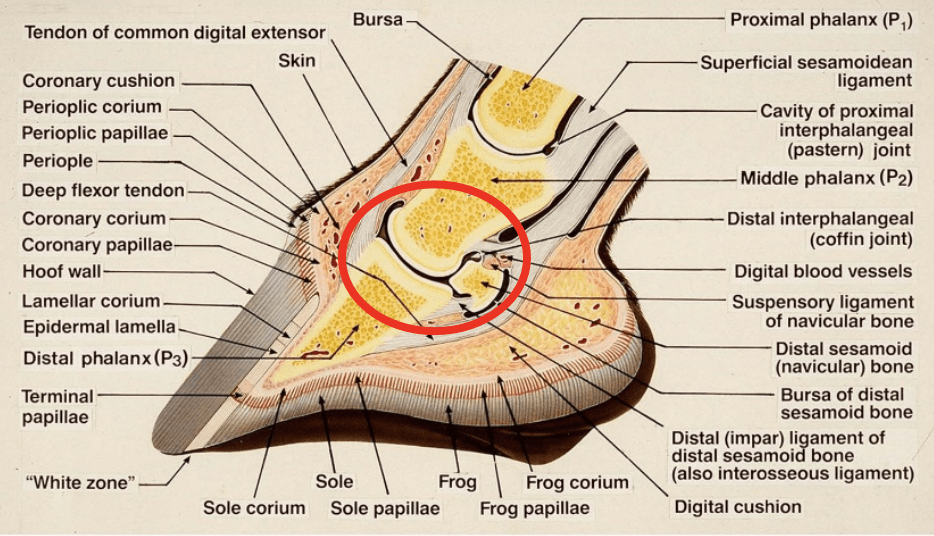
The Hoof The equine hoof is unique as it is comprised of a group of biological structures (anatomy) that follow the laws of biomechanics. Therefore, if the veterinarian and farrier know the anatomy of the equine foot combined with an understanding of the biomechanics and good basic farriery principles, proper physiological farriery can be consistently applied (see Figure 1A and 1B). There are three important aspects of farriery used to keep the horse sound, beginning with the appropriate foot trim, along with the correct size and placement of the horseshoe.
Fig. 1A – Illustration shows the biological structures of the hoof and the biomechanical focus.
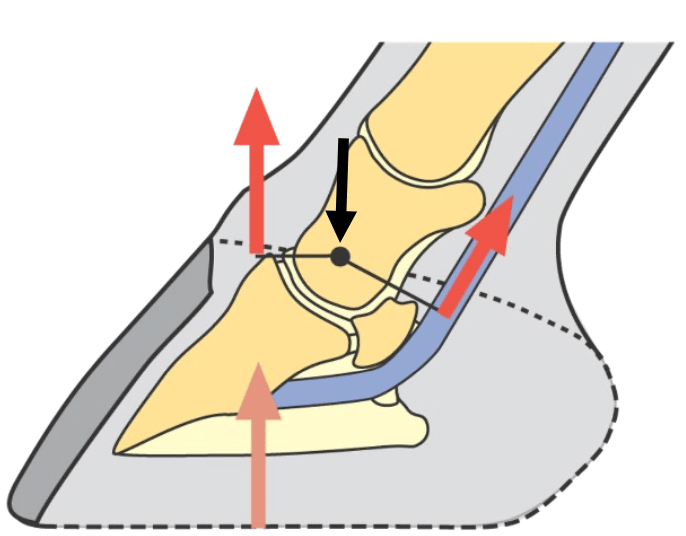
Fig. 1B – Biomechanical properties of the foot. (Black arrow is COR). Note the moments on either side of the COR.
The farrier session begins with an evaluation of the conformation of each foot. This means viewing the foot from the front, the side, and behind to observe the height of the heel bulbs (see Figure 2). It is important for the clinician to observe the horse in motion to see whether the horse’s foot lands flat or slightly heel first, which is desired. If the horse lands markedly heel first with a toe flip, it is a sign the heels have migrated dorsally (toward the front), decreasing the ground surface in the palmar section of the foot, or the size of the shoes is too small. The foot that lands toe first is an indication that the musculotendinous unit of the deep digital flexor tendon is shortened or the horse is experiencing palmar foot pain. Lastly, the foot should be observed for an asymmetrical landing pattern that is dictated by limb conformation because, if severe, a heel bulb can be displaced proximally resulting in the foot conformation termed “sheared heels.”
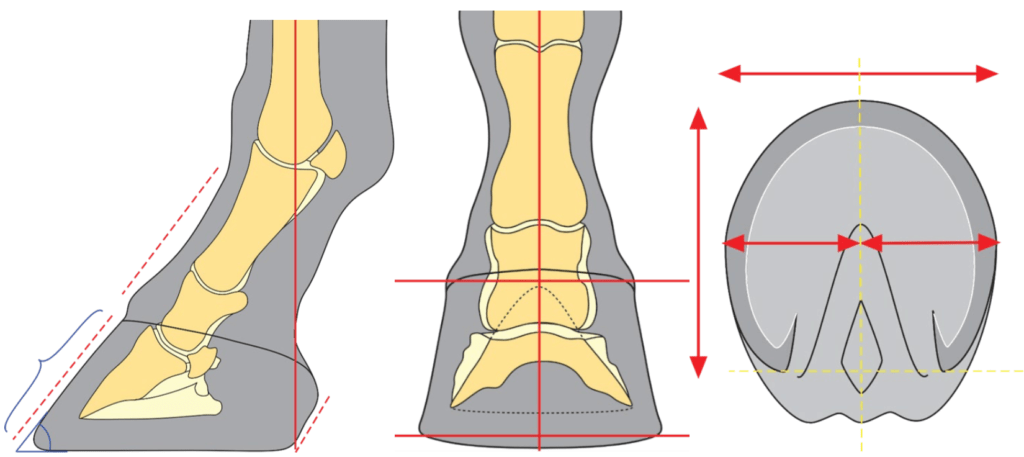
Fig. 2 – Illustrations of what is considered good foot conformation. Lateral view shows straight bony alignment of the digit and a parallel hoof-pastern axis. DP view shows straight alignment of the digit and a line across the coronet is parallel with a line on the ground. Ground surface of the foot shows good proportions on either side of a line across the widest part of the foot. Note foot is basically as wide as it is long.
The Trim The use of guidelines or landmarks when approaching the trim provides consistent, repeatable results that can be used on each foot regardless of the conformation. The three guidelines used are: 1. Trimming the foot to achieve a straight or parallel hoof-pastern axis, 2. using the widest part of the foot, which correlates closely with the center of rotation, and 3. trimming the palmar foot (heels) to the base of the frog or to where the heels of the hoof capsule and the frog are on the same plane (see Figure 3A and 3B). A closer look at these three guidelines, which are all interrelated, will help to show their importance.
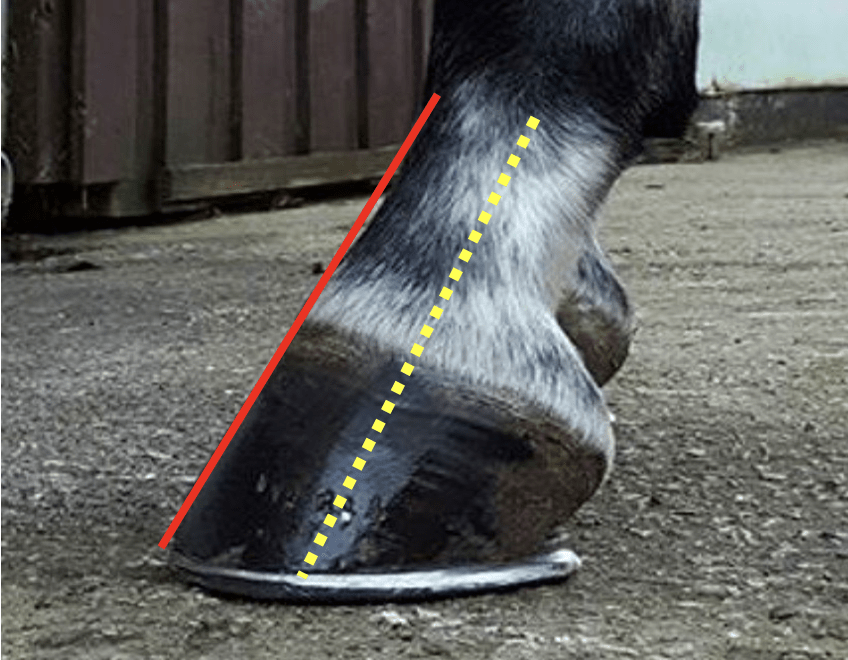
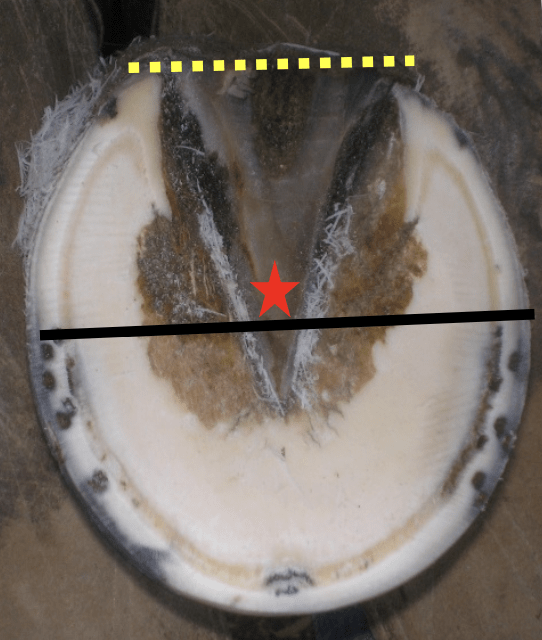
Fig. 3A – Yellow dotted line shows the bony alignment of the digit. Red line shows the straight hoof-pastern axis.
Fig. 3B – Black line is the widest part of the foot and the yellow dotted line shows the heels trimmed to the base of the frog. Star is position of COR.
1. If the dorsal (front) surface of the pastern bone and the dorsal surface of the hoof are parallel or form a straight line, then the bones of the digit (in the hoof) are in a straight line, and the force from the weight of the horse will go through the center of the joint. Furthermore, and equally important, if the hoof-pastern axis is straight, the weight will be distributed evenly on the bottom or the solar surface of the foot.
2. The second guideline is the center of rotation (COR). The COR is located a few millimeters palmar (behind) the widest part of each foot. This guideline allows the farrier to apply the appropriate biomechanics to each foot. The foot is trimmed in approximate proportions on either side of the widest part of the foot, which addresses the moments on either side of the COR and provides biomechanical efficiency.
3. Lastly, the palmar section of the foot is trimmed to the base of the frog or trimmed such that the heels of the hoof capsule and the frog are on the same plane. Adherence to this guideline keeps the soft tissue structures (frog, digital cushion, ungula cartilages) within the hoof capsule, which is necessary to absorb concussion and dissipate the energy of impact (see Figure 4). It is important to remember that heels do not grow tall; they grow forward. If the heels migrate forward, the soft tissue structures will be forced in a palmar direction out of the hoof capsule. Furthermore, as the heels migrate forward, the weight is placed on the bone via the lamellae thus bypassing the soft tissue structures of the foot. Allowing the heels to migrate forward also decreases the ground surface of the foot. Two examples of this guideline are shown in Figures 5A, 5B and 6A, 6B where the palmar foot was managed appropriately, and a size larger shoe was applied.
Fig. 4 – Illustration shows the relationship between the osseous and soft tissue structures within the hoof capsule. If heels migrate dorsally, load is transfer to the bone (note arrow).
Fig. 5A – Heels have migrated dorsally and red circle shows the soft tissu structures displaced proximally out of the hoof capsule.
Fig. 5B – Same foot after the heels have been trimmed and a larger shoe has been applied.
Fig. 6A – Heels are low and have migrated dorsally with the soft tissue structures displaced proximally out of the hoof capsule.
Fig. 6B – Same fott after the heels have been trimmed and a larger showe and heel elevation applied.
The three guidelines described here can be applied to any foot and can serve as a basis for maintaining a healthy foot and a basic starting point for applying farriery to a horse with poor foot conformation or one with a distorted hoof capsule. Figures 7A and 7B illustrate a hoof where all three of these guidelines have been applied.
Fig. 7A – The three guidelines applied to the foot. Note the proportions on either side of the widest part (black line) of the foot.
Fig. 7B – Shows the length of the shoe and the wide expanse of the shoe creating a platform under the palmar section of the foot.
Thoughts From Dr. Stephen O’Grady Most competition horses now show year-round instead of on a seasonal basis. My observation is based on years of experience regarding the farriery performed on these horses. Many of these horses are given a rest from competition prior to leaving for Wellington for the winter show season. Many horses arrive with very reasonable foot conformation. However, upon arrival, horses are often shod with various specialty shoes, wedges, pads, pour-ins, etc., as a means of protection and perhaps to enhance their performance.
As the season progresses and the workload becomes more intense, the sole thickness starts to decrease, and the feet become softer from multiple baths. Now the farriery that was applied for protection at the onset may be causing pressure on the thinner, softer structures of the foot, thus becoming somewhat detrimental. The horses continue to be trimmed and shod on a monthly basis, and the farrier may not be aware of the change in the integrity of the hoof structures, especially the sole, and perhaps some horses may be over-trimmed. As the season progresses into March, the structures of the foot deteriorate further as a result of the workload. Many horses begin to become foot sore. At this point, the farrier options become limited because all the protective methodology was already used at the beginning of the season.
One recommendation would be to refrain from trimming the sole (trade the hoof knife for a wire brush), create ground surface in the palmar foot with a rasp, and decrease toe length vertically from the dorsal section of the foot to preserve mass. Always remember that adequate breakover in the shoe is important, as it decreases the stress in the deep digital flexor tendon and decreases the moment about the distal interphalangeal joint, both of which preserve sole thickness.
I remember the words of Joe Pierce when I was an apprentice learning the farrier trade many years ago, “No one will know if you leave the last few rubs of the rasp on the foot, but everyone will know if you take a few too many rubs!”
Palm Beach Equine Clinic offers a farriery consultation service to both veterinarians and farriers. This unique service provides a second opinion or simply “another set of eyes” available to both professions when treating difficult farriery cases. Please call 561-793-1599 or visit equineclinic.com for more information.
Equine ulcers have long been a common concern for horse owners. Our understanding of ulcers has dramatically improved over time through medical advancement, and there is currently more nuance to the diagnostics, treatment, and management of horses suffering from these internal sores. Gastroscopy and ultrasound have become more readily available, and their increased accessibility have allowed non-specialty practitioners more experience and a greater comfort level with these tools. These developments throughout the industry have led to more animals being correctly diagnosed and appropriately treated.
Jordan Lewis, DVM of Palm Beach Equine Clinic (PBEC) sees a variety of equine ulcer cases. She breaks them down into three categories: gastric ulcer disease of the squamous mucosa, gastric ulceration of the glandular mucosa, and colon ulcers of the right dorsal colon.
Equine gastric ulcer disease of the squamous mucosa refers to the ulcers found on the stomach’s inner lining closer to the esophagus. They are primarily caused by exposure to stomach acid and vary in severity depending on the amount of time the stomach’s lining has been in contact with the stomach acid.
“We often see this increased stomach acid exposure with the squamous mucosa in performance horses due to the mechanical aspects of exercise and abdominal pressure,” Dr. Lewis described. “The increase in acid production and contact time can also be seen in fasting animals and animals with delayed gastric emptying or slowed motility.”
Glandular mucosa describes the stomach lining around the pyloric region closer to the intestines. Ulcers found here are typically caused by a decrease in mucosal blood-flow as well as a decrease in mucus production, which normally serves as a protective barrier for the stomach lining. Stress and non-steroidal anti-inflammatory drugs (NSAIDS) such as phenylbutazone (“bute”) or flunixin meglumine (“Banamine®”) are the usual culprits in this case.
Similarly, ulcers found in the colon are also usually caused by stress and NSAID administration, leading to a decrease in the mucosal wall protection resulting in ulceration and inflammation.
“In some cases with colon ulcers of the right dorsal colon, we see minimal thickening noted on the right abdominal wall, but other times it can be more severe thickening with more ominous clinical signs of colic, fever, hypoalbuminemia (protein loss), ventral and limb edema, and diarrhea,” detailed Dr. Lewis.
The tricky thing about ulcers is that they do not always present with the same symptoms in every horse. It can be difficult to know when it’s time to be a little more invasive in order to take a closer look at a horse’s digestive system. At a minimum, persistent symptoms warrant a veterinarian consultation.
“The range of symptoms can vary from mild to severe,” Dr. Lewis explained. “The horse might be being a picky eater, or they might exhibit moderate to severe colic symptoms like signs of abdominal discomfort such as pawing or rolling. Even still, some horses present with the only outward sign being poor performance.”
Dr. Lewis uses varying diagnostic tools for a complete understanding of the affliction. Sometimes she will perform the Succeed test, which is a fecal test that generally helps indicate the presence of ulcers. Another option is to perform a gastroscopy with a three-meter endoscope to see the stomach where both forms of gastric ulcers are found. Ultrasound is the primary diagnostic tool to look for thickening of the right dorsal colon wall indicating ulceration in the colon. Basic bloodwork to determine total albumin, a protein made by the liver, also helps indicate more severe cases of colon ulcers.
Once a horse has been diagnosed with ulcers of any variety it’s important to begin treatment, especially since horses suffering from ulcers are predisposed to colic. Because each type of ulcer disease has a different underlying cause, the treatment protocol and medications are also different.
Though omeprazole paste used to be thought of as the cure-all, today we know that it is only part of the puzzle. Dr. Lewis recommends an omeprazole paste for at least a four-week period and uses other medications in conjunction with this depending on what type of ulcer she is treating. For horses that have ulcers of the squamous mucosa experiencing more severe, colic-like symptoms, Dr. Lewis adds a dose of sucralfate before meals to the protocol. If she finds ulcers in the glandular and pyloric region of the stomach, misoprostol and prostaglandin analog is used. For ulcers of the right dorsal colon, sucralfate is used as a coating agent while misoprostol is used as a treatment.
In addition to medication, some lifestyle adjustments can aid in maintaining an ulcer-free digestive tract. “It’s helpful if we can provide a more natural, less stressful environment for these horses with continuous grazing on pasture or hay as well as more turnout,” stated Dr. Lewis.
She continued, “Horses with gastric ulcers do well on adding alfalfa hay as a buffering agent before a grain meal, while horses with colon ulcers do well on a low-bulk diet, meaning less forage and a more complete feed-based pellet. Adding a psyllium-based supplement can be helpful for these horses too.”
Even with the best curative efforts, some horses can continue to suffer from ulcers, underscoring the importance of monitoring your horse for any changes even after treatment. Because sport horses have an increased likelihood of developing gastric ulcers due to exercise, their constant work also increases the odds of them have recurring ulcers. Personality and demeanor also play a part.
“Horses that have recurrent ulcer disease tend to be horses that internalize more and are stressed easily,” said Dr. Lewis.
She highlighted some additional measures that can be taken to help continuously protect the stomach’s lining, noting the importance of a regulated diet and more opportunity to relax, as well as treatment with a prophylactic dose of omeprazole paste.
If you think your horse feels a little off from their normal behavior, it might be time to discuss different diagnostic options with your veterinarian. Trust your gut – it might just help your horse’s too.