Category: Surgery
A recent popular post on PBEC’s social media was about retired Davie County, FL, police horse Charlie, who injured himself in true equine fashion – spectacularly and with no one knowing how – during the night while turned out in a field. Charlie was adopted by the mother of one of the Davie County police officers who also works for the Sheriff’s Department. They brought Charlie to PBEC to repair a large laceration on his side.

Dr. Michelle Maguire was on hand to care for Charlie and explained the steps it took to get him back to healing. Dr. Maguire and her team administered intravenous sedation in order to repair with him standing up then injected local anesthesia around the circumference of the laceration, which measured approximately 12 by 18 inches.
“This case was particularly challenging because it was a very large area with multiple flaps and went through many layers, including skin, subcutaneous tissue, and the muscle layers overlying the thorax,” said Dr. Maguire. “Luckily there was no penetration into the thoracic cavity.”
Dr. Maguire used walking sutures to close the laceration, extending from the skin flap’s deep dermis to the underlying fascia of the body wall. This approach helps eliminate
dead space to help prevent seroma formation and infection, reduce skin tension, promote wound closure, and lower the risk of dehiscence, a surgical complication where a wound ruptures along the incision after surgery.
Because the skin can’t handle tension, you can’t just suture the skin itself. Dr. Maguire also used a Jackson Pratt drain, a commonly used surgical drain that provides a constant, low suction to pull fluid from a surgical incision site to decrease swelling and reduce the risk of infection. The drain consists of a thin, rubber tube and a soft, round squeeze bulb, or “grenade” on the end that maintains negative pressure and allows for an active drainage system.

Dr. Maguire noted that Charlie’s prognosis is very good, and he is expected to make a full recovery. He has been doing well at home, and the wound has held together without dehiscence.
She added, “The aftercare protocol was a course of systemic antibiotics and anti-inflammatories, along with maintaining a compressive for the first two weeks postoperatively until skin sutures were removed.
“The horse handled everything very well,” she continued. “He was in pain the first day postoperatively, but as the inflammation subsided, he was a normal happy horse.”
The team at Palm Beach Equine Clinic is happy to report that Charlie is back home grazing. While he will have a scar, it won’t affect his quality of life, and he will have quite a story to tell his friends!
By Alice Collins / Jump Media
Originally from Corrientes in the north of Argentina, Lujan Montiel completed her veterinary degree in her home country in 2016, then specialized in treating polo ponies before joining the intern program at Palm Beach Equine Clinic (PBEC).

What is your background with horses?
Over the past eight years, I have worked primarily with polo horses, focusing on their care and management in a field setting — a very different scenario from Wellington and of course from a hospital environment.
When and why did you decide you wanted to become an intern at Palm Beach Equine Clinic?
Since 2023 I have been in contact with PBEC, exploring the possibility of joining the 2024-2025 internship program. My interest in this internship stems from a desire to broaden my expertise and gain a comprehensive view of equine medicine. I aim to specialize further by integrating the intensive care practices performed at the clinic, in addition to learning from the high-level professionals and advanced technology that the hospital offers for both hospitalized and outpatients.

What does the internship program involve?
The program involves rotations through all areas of equine veterinary medicine, including internal medicine, surgery, anesthesia, sport medicine, ophthalmology, and dentistry. The structured rotations, changing every two weeks, provide a unique opportunity to develop skills across multiple disciplines.
What does a typical day look like for you at PBEC?
A typical day at PBEC begins with checking all my patients, performing physical exams, and updating their medical notes. At 8:30 a.m., we have rounds where we discuss cases with the doctors. Occasionally, we have scheduled surgeries, which always start at 9 a.m. Depending on the day and the rotation I’m in, I could be working in surgery, anesthesia, in the hospital, or ambulatory work with one of the clinicians. Therefore, each day can be quite variable and diverse, offering a broad range of experiences.

What aspects of equine medicine interest you most, and what types of cases do you find most rewarding?
The area of veterinary medicine that most interests me is internal medicine. Since my arrival in late June, I have had the privilege of treating a wide variety of cases, including laminitis, colic, neurological patients, diarrheas, and endotoxemia cases, among others.
What is one of the most interesting cases you have worked on?
The cases that I’ve found most interesting and educational have been colic cases due to their variety and the protocol-based management that the clinic employs. There were a series of four colic cases (one next to the other), and all of them were resolved surgically. All of these cases involved a very rare condition called mesocecum entrapment, which prompted significant research into this topic at the clinic.

What’s your favorite part of the job/the biggest thing you have learned?
What I enjoy most about working at PBEC is the willingness of the clinicians to share their expertise in various fields, whether it’s sports medicine, surgery, anesthesia, or internal medicine. Their dedication to teaching ensures that the internship is as rewarding and beneficial as possible, allowing us to truly make the most out of this intensive year of work. Additionally, I have been fortunate to work with a group of interns who have excellent values of camaraderie, making everything lighter and easier when things get busy at the clinic.
When not at PBEC, what do you enjoy doing in your free time?
During my days off, I try to explore the surrounding areas of Wellington, including the beach, as it’s a new country for me, and I love taking the opportunity to enjoy the coastline.
To learn more about the full range of services on offer at Palm Beach Equine Clinic, call 561-793-1599 or visit www.EquineClinic.com.
By Alice Collins / Jump Media
Wellington, FL – Miss Miami is one of Miami’s longest-serving and most-valued police horses, having joined the team 21 years ago and been through six police chiefs. In the early spring of 2024 at the age of 26, Miami Police Department (PD) had begun to wind down her workload and prepare her for retirement. However, on April 10 Miss Miami looked uncomfortable, and officers called their veterinarian.
“She was not feeling good, and it looked like colic,” explained Lieutenant Redondo of Miami PD. “The vet came and saw she was in distress and said we’d probably have to do surgery. They couldn’t do it and referred us to Palm Beach Equine Clinic [PBEC].”
Miss Miami was driven straight to PBEC in Wellington, FL, where the team carried out a physical exam, blood work, nasogastric intubation, an ultrasound, abdominocentesis, and a rectal exam. Their findings were consistent with a surgical lesion, and she was diagnosed with a strangulating lipoma, a small, benign, fatty tumor that develops within the abdomen and occasionally develops a long, string-like stalk. The lipoma and stalk can wrap around a part of the horse’s digestive system, cutting off the blood supply and resulting in death of that section of intestine.

On the day she arrived at PBEC, Miss Miami was taken to emergency surgery after an initial evaluation and operated on by Dr. Weston Davis DVM, DACVS, who ended up performing a resection and anastomosis, which is where a part of intestine is removed and the two ends are rejoined.
“Miss Miami was routinely induced under general anesthesia; the abdomen was clipped and aseptically prepared for surgery,” explained Davis, who is a native of South Florida and whose father was also a veterinarian. “A midline incision was created, and exploration revealed a large segment of mid-jejunum [the middle part of the small intestine] that appeared to have been strangulated by the stalk of a strangulating lipoma.”
The portion of the small intestine affected was no longer viable, so Davis removed the two-foot long segment of jejunum. Miss Miami’s abdominal incision was then closed with absorbable sutures in the deeper layers and stainless-steel staples in the skin.
Miss Miami was given intravenous fluid therapy including pain relief, electrolytes, anti-inflammatories, antibiotics, and gastroprotectants. She recovered from the anesthesia without incident, and a large abdominal support bandage was applied in recovery.

She was not yet out of the woods, however. Miss Miami’s forelimb digital pulses were mildly elevated in the first 36 hours after the operation. She was managed with digital cryotherapy, and frog supports were applied to both front feet. Her appetite was also diminished following surgery, and she was fed via nasogastric intubation until her appetite began to increase. At that point, her rations were given normally, and the quantity was gradually increased. Her digital pulses returned to normal.
After a week at PBEC, Miss Miami was bright, with a good appetite, passing normal manure, and walking comfortably. She was ready to be released back into the care of Miami PD. Their local veterinarian oversaw the removal of Miss Miami’s stitches a week later, and her belly bandage was reapplied. The Miami PD team was also given four daily exercises by PBEC for Miss Miami to start at home two weeks after surgery to help support her recovery: barrel lifts, butt tucks, stepping backwards, and walking over poles.

“She would have died without the surgery,” stated Redondo. “She has recovered really well. She is still here with us in Miami, but we have started the paperwork to retire her to farmland up in North Florida. Everybody around here knows her and loves her; she’s one of our most famous horses. She’s been here longer than I have, and she’s one of the horses that we liked to use on the regular. Having a horse that already knows the job and is used to all the traffic and loud noises makes it easy, so we are going to miss her.
“The fact that the department agreed to take care of a horse who is old or not being ridden anymore says a lot, and the fact that PBEC took care of her was so great,” he concluded.

PBEC’s kindness and swift action ensured that Miss Miami will now be able to enjoy the retirement she deserves after her years of loyal service. If you or your veterinarian would like to learn more about Palm Beach Equine Clinic and how it can help your horse, call 561-793-1599 or visit www.EquineClinic.com.

Palm Beach Equine Clinic is one of the foremost equine surgical centers in the world with three board-certified surgeons on staff, led by Dr. Weston Davis. As a busy surgeon, Dr. Davis has seen many horses with the dreaded “kissing spines” diagnosis come across his table. Two of his most interesting success stories featured horses competing in the disciplines of barrel racing and dressage.
Flossy’s Story

The words “your horse needs surgery” are ones that no horse owner wants to hear, but to Sara and Kathi Milstead, it was music to their ears. In 2016, Sara – who was 17 years old at the time and based in Loxahatchee, Florida – had been working for more than a year to find a solution to her horse’s extreme behavioral issues and chronic back pain that could not be managed. Her horse Two Blondes On Fire, a then-eight-year-old Quarter Horse mare known as “Flossy” in the barn, came into Sara’s life as a competitive barrel racer. But shortly after purchasing Flossy, Sara knew that something wasn’t right.
“We tried to do everything we could,” said Sara. “She was extremely back sore, she wasn’t holding weight, and she would try to kick your head off. We tried Regu-Mate, hormone therapy, magna wave therapy, injections, and nothing helped her. We felt that surgery was the best option instead of trying to continue injections.”
At the time, Sara and her primary veterinarian, Dr. Jordan Lewis of Palm Beach Equine Clinic (PBEC), brought Flossy to PBEC for thorough diagnostics. They determined Flossy had kissing spines.
Kissing Spines Explained
In technical terms, kissing spines are known as overriding or impinging dorsal spinous processes. The dorsal spinous process is a portion of bone extending dorsally from each vertebra. Ideally, the spinous processes are evenly spaced, allowing the horse to comfortably flex and extend its back through normal positions. With kissing spines, two or more vertebrae get too close, touch, or even overlap in places. This condition can lead to restrictions in mobility as well as severe pain, which ultimately can lead to back soreness and performance problems.
“The symptoms can be extremely broad,” acknowledged Dr. Davis. “[With] some of the horses, people will detect sensitivity when brushing over the topline. A lot of these horses get spasms in their regional musculature alongside the spinous processes.” A significant red flag is intermittent, severe bad behavior, such as kicking out, bucking, and an overall negative work attitude, something that exactly described Flossy.

Lakota’s Story
With dressage horse Lakota owned by Heidi Degele, there were minimal behavior issues, but Degele knew there had to be something more she could do to ease Lakota’s pain.
“As his age kicked in, it was like you were sitting on a two-by-four,” Heidi said of her horse’s condition. “I knew his back bothered him the most because with shockwave he felt like a different horse; he felt so supple and he had this swing in his trot, so I knew that’s what truly bothered him.” Though she could sense the stiffness and soreness as he worked, he was not one to rear, pin his ears, or refuse to work because of the pain he was feeling.
Heidi turned to Dr. Davis, who recommended a surgical route, an option he only suggests if medical treatment and physical therapy fail to improve the horse’s condition. “Not because the surgery is fraught with complications or [tends to be] unsuccessful,” he said, “but for a significant portion of these horses, if you’re really on top of the conservative measures, you may not have to opt for surgery.
“That being said, surgical interventions for kissing spines have very good success rates,” added Dr. Davis. In fact, studies have shown anywhere from 72 to 95 percent of horses return to full work after kissing spines surgery.
After Lakota made a successful recovery from his surgery in 2017, he has required no maintenance above what a typical high-level performance horse may need. Heidi attributes his success post-surgery to proper riding, including ground poles that allow him to correctly use his back, carrot stretches, and use of a massage blanket, which she has put into practice with all the horses at her farm. Dr. Davis notes that proper stretching and riding may also prolong positive effects of injections while helping horses stay more sound and supple for athletic activities.
Lakota, who went from Training Level all the way up through Grand Prix, is now used by top working students to earn medals in the Prix St. Georges, allowing them to show off their skills and earn the qualifications they need to advance their careers.

Flossy’s Turnaround
Flossy was found to have dorsal spinous process impingement at four sites in the lower thoracic vertebrae. Dr. Davis performed the surgery under general anesthesia and guided by radiographs, did a partial resection of the affected dorsal spinous processes (DSPs) to widen the spaces between adjacent DSPs and eliminate impingement.
Sara took her time bringing Flossy back to full work. Within days of the surgery, Sara saw changes in Flossy, but within six months, she was a new horse.
“Surgery was a big success,” said Sara. “Flossy went from a horse that we used to dread riding to the favorite in the barn. It broke my heart; she was just miserable. I didn’t know kissing spines existed before her diagnosis. It’s sad to think she went through that pain. She’s very much a princess, and all of her behavioral problems were because of pain. Now my three-year-old niece rides her around.”


Sara and Flossy have returned to barrel racing competition as well, now that Sara graduated from nursing school, and have placed in the money regularly including two top ten finishes out of more than 150 competitors.
“I can’t even count the number of people that I have recommended Palm Beach Equine Clinic to,” said Sara. “Everyone was really great and there was excellent communication with me through every step of her surgery and recovery.”
By finding a diagnosis for Flossy and a way to ease her pain, Sara was able to discover her diamond in the rough and go back to the competition arena with her partner for years to come.
What To Expect After the Unexpected Strikes
Featured on Horse Network
Every owner dreads having to decide whether or not to send their horse onto the surgical table for colic surgery. For a fully-informed decision, it is important that the horse’s owner or caretaker understands what to expect throughout the recovery process.
Palm Beach Equine Clinic (PBEC) veterinarian Weston Davis, DVM, DACVS, assisted by Sidney Chanutin, DVM, has an impressive success rate when it comes to colic surgeries, and the PBEC team is diligent about counseling patients’ owners on how to care for their horse post-colic surgery.

“After we determine that the patient is a strong surgical candidate, the first portion of the surgery is exploratory so we can accurately define the severity of the case,” explained Dr. Davis. “That moment is when we decide if the conditions are positive enough for us to proceed with surgery. It’s always my goal to not make a horse suffer through undue hardship if they have a poor prognosis.”
Once Dr. Davis gives the green light for surgical repair, the surgery is performed, and recovery begins immediately.
“The time period for the patient waking up in the recovery room to them standing should ideally be about 30 minutes,” continued Dr. Davis. “At PBEC, we do our best to contribute to this swift return by using a consistent anesthesia technique. Our team controls the anesthesia as lightly as we can and constantly monitors blood pressure. We administer antibiotic, anti-inflammatory, anti-endotoxic drugs, and plasma to help combat the toxins that the horse releases during colic. Our intention in the operating room is to make sure colic surgeries are completed successfully, but also in the most time-efficient manner.”
Colic surgery recovery often depends on the type and severity of the colic. At the most basic level, colic cases can be divided into two types – large intestine colic and small intestine colic – that influence the recovery procedures and outlook.
Large intestinal colic or impaction colic is characterized by the intestine folding upon itself with several changes of direction (flexures) and diameter changes. These flexures and diameter shifts can be sites for impactions, where a firm mass of feed or foreign material blocks the intestine. Impactions can be caused by coarse feeds, dehydration, or an accumulation of foreign materials such as sand.
Small intestinal colic or displacement colic can result from gas or fluid distension that results in the intestines being buoyant and subject to movement within the gut, an obstruction of the small intestine, or twisting of the gut. In general, small intestinal colics can be more difficult than large intestinal colics when it comes to recovery from surgery.
“Many people do assume that after the colic surgery is successfully completed their horse is in the clear,” said Dr. Chanutin. “However, during the first 24 to 48 hours after colic surgery, there are many factors that have to be closely monitored.
“We battle many serious endotoxic effects,” continued Dr. Chanutin. “When the colon isn’t functioning properly, microbial toxins are released inside the body. These microbials that would normally stay in the gastrointestinal tract then cause tissue damage to other bodily systems. We also need to be cognizant of the possibility of the patient developing laminitis, a disseminated intervascular coagulation (overactive clotting of the blood), or reflux, where a blockage causes fluids to back up into the stomach.”

Stages after surgery
Immediately Post-Surgery
While 30 minutes from recumbent to standing is the best-case scenario, Dr. Davis acknowledges that once that time period passes, the surgical team must intervene by encouraging the horse to get back on its feet.
Once a horse returns to its stall in the Equine Hospital at PBEC, careful monitoring begins, including physical health evaluations, bloodwork, and often, advanced imaging. According to Dr. Davis, physical exams will be conducted at least four times per day to evaluate the incision and check for any signs of fever, laminitis, lethargy, and to ensure good hydration status. An abdominal ultrasound may be done several times per day to check the health of the gut, and a tube may be passed into the stomach to check for reflux and accumulating fluid in the stomach.
“The horse must regularly be passing manure before they can be discharged,” said Dr. Chanutin. “We work toward the horse returning to a semi-normal diet before leaving PBEC. Once they are at that point, we can be fairly confident that they will not need additional monitoring or immediate attention from us.”
Returning Home
Drs. Davis and Chanutin often recommend the use of an elastic belly band to support the horse’s incision site during transport from the clinic and while recovering at home. Different types of belly bands offer varying levels of support. Some simply provide skin protection, while others are able to support the healing of the abdominal wall.

Two Weeks Post-Surgery
At the 12-to-14-day benchmark, the sutures will be removed from the horse’s incision site. The incision site is continuously checked for signs of swelling, small hernias, and infection.
At-Home Recovery
Once the horse is home, the priority is to continue monitoring the incision and return them to a normal diet if that has not already been accomplished.
The first two weeks of recovery after the horse has returned home is spent on stall rest with free-choice water and hand grazing. After this period, the horse can spend a month being turned out in a small paddock or kept in a turn-out stall. They can eventually return to full turnout during the third month. Hand-walking and grazing is permittable during all stages of the at-home recovery process. After the horse has been home for three months, the horse is likely to be approved for riding.
Generally, when a horse reaches the six-month mark in their recovery, the risk of adverse internal complications is very low, and the horse can return to full training under saddle.
When to Call the Vet?
Decreased water intake, abnormal manure output, fever, pain, or discomfort are all signals in a horse recovering from colic surgery when a veterinarian should be consulted immediately.
Long-Term Care
Dr. Davis notes that in a large number of colic surgery cases, patients that properly progress in the first two weeks after surgery will go on to make a full recovery and successfully return to their previous level of training and competition.
Depending on the specifics of the colic, however, some considerations need to be made for long-term care. For example, if the horse had sand colic, the owner would be counseled to avoid sand and offer the horse a selenium supplement to prevent a possible relapse. In large intestinal colic cases, dietary restrictions may be recommended as a prophylactic measure. Also, horses that crib can be predisposed to epiploic foramen entrapment, which is when the bowel becomes stuck in a defect in the abdomen. This could result in another colic incident, so cribbing prevention is key.
Generally, a horse that has fully recovered from colic surgery is no less healthy than it was before the colic episode. While no one wants their horse to go through colic surgery, owners can rest easy knowing that.
“A lot of people still have a negative association with colic surgery, in particular the horse’s ability to return to its intended use after surgery,” said Dr. Davis. “It’s a common old-school mentality that after a horse undergoes colic surgery, they are never going to be useful again. For us, that situation is very much the exception rather than the rule. Most, if not all, recovered colic surgery patients we treat are fortunate to return to jumping, racing, or their intended discipline.”
When the Bone Breaks
Palm Beach Equine Clinic is Changing the Prognosis for Condylar Fracture Injuries
Palm Beach Equine Clinic is changing the prognosis for condylar fracture injuries in race and sport horses. Advances in diagnostic imaging, surgical skillset, and the facilities necessary to quickly diagnose, treat, repair, and rehabilitate horses with condylar fractures have improved dramatically in recent years.
Photo by Jump Media
Most commonly seen in Thoroughbred racehorses and polo ponies, a condylar fracture was once considered a career-ending injury. Today, however, many horses fully recover and return to competing in their respective disciplines.
What is a Condylar Fracture?
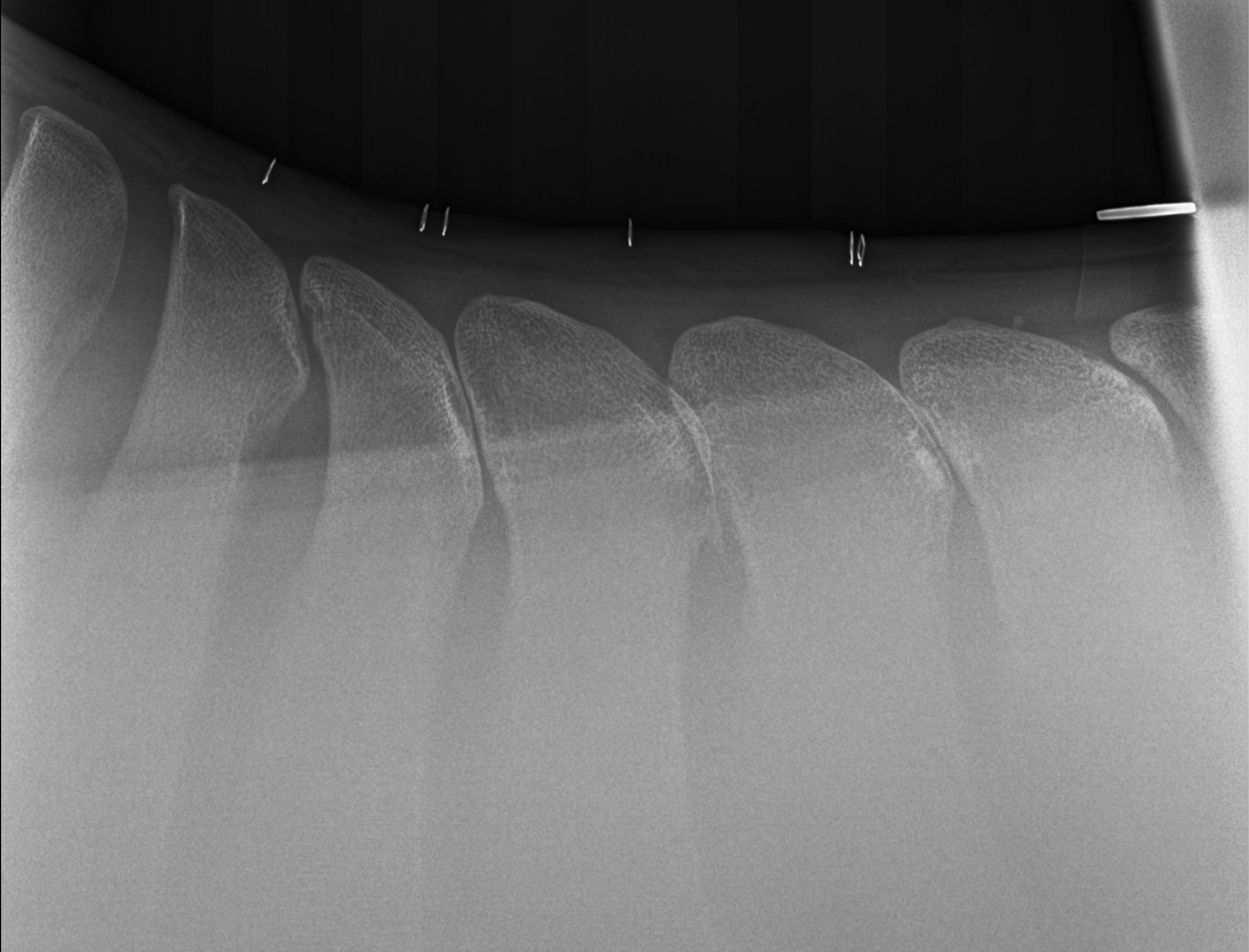
A condylar fracture is a repetitive concussive injury that results in a fracture to the cannon bone above the fetlock due to large loads transmitted over the cannon bone during high-speed exercise. On a radiograph, a condylar fracture appears as a crack that goes laterally up the cannon from the fetlock joint and out the side of the bone, essentially breaking off a corner of the cannon bone, sometimes up to six inches long.

“A condylar fracture is a disease of speed,” said Dr. Robert Brusie, a surgeon at Palm Beach Equine Clinic who estimates that he repairs between 30 and 50 condylar fractures per year. “A fracture to the left lateral forelimb is most common in racehorses as they turn around the track on a weakened bone and increased loading.”

Condylar fractures are further categorized into incomplete and non-displaced (the bone fragment hasn’t broken away from the cannon bone and is still in its original position), or complete and displaced (the fragment has moved away from the cannon bone itself and can often be visible under the skin).
Additionally, condylar fractures can occur laterally or medially. According to fellow Palm Beach Equine Clinic surgeon Dr. Weston Davis, most condylar fractures tend to be lateral on the outside condyle (a rounded projection on a bone, usually for articulation with another bone similar to a knuckle or joint).
“Most lateral condylar fractures are successfully repaired,” said Dr. Davis. “Medial condylar fractures tend to be more complicated configurations because they often spiral up the leg. Those require more advanced imaging and more advanced techniques to fix.”
What is the Treatment?
The first step in effectively treating a condylar fracture through surgery is to accurately and quickly identify the problem. Board-certified radiologist Dr. Sarah Puchalski utilizes the advanced imaging services at Palm Beach Equine Clinic to accomplish exactly this.
“Stress remodeling can be detected early and easily on nuclear scintigraphy before the horse goes lame or develops a fracture,” said Dr. Puchalski. “Early diagnosis of stress remodeling allows the horse to be removed from active race training and then return to full function earlier. Early diagnosis of an actual fracture allows for repair while the fracture is small and hopefully non-displaced.”

Photo by Jump Media
Once the injury is identified as a condylar fracture, Palm Beach Equine Clinic surgeons step in to repair the fracture and start the horse on the road to recovery. Depending on surgeon preference, condylar fracture repairs can be performed with the horse under general anesthesia, or while standing under local anesthesia. During either process, surgical leg screws are used to reconnect the fractured condyle with the cannon bone.
“For a small non-displaced fracture, we would just put in one to two screws across the fracture,” explains Dr. Davis. “The technical term is to do it in ‘lag fashion,’ such that we tighten the screws down heavily and really compress the fracture line. A lot of times the fracture line is no longer visible in x-rays after it is surgically compressed. When you get that degree of compression, the fractures heal very quickly and nicely.”
More complicated fractures, or fractures that are fully displaced, may require additional screws to align the parts of the bone. For the most severe cases of condylar fractures, a locking compression plate with screws is used to stabilize and repair the bone.
Palm Beach Equine Clinic surgeon Dr. Jorge Gomez approaches a non-displaced condylar fracture while the horse is standing, which does not require general anesthesia.

“I will just sedate the horse and block above the site of the fracture,” said Dr. Gomez. “Amazingly, horses tolerate it really well. Our goal is always to have the best result for the horse, trainers, and us as veterinarians.”
According to Dr. Gomez, the recovery time required after a standing condylar fracture repair is only 90 days. This is made even easier thanks to a state-of-the-art standing surgical suite at Palm Beach Equine Clinic. The four-and-a-half-foot recessed area allows doctors to perform surgeries anywhere ventral of the carpus on front legs and hocks on hind legs from a standing position. Horses can forgo general anesthesia for a mild sedative and local nerve blocks, greatly improving surgical recovery.
“A condylar fracture was once considered the death of racehorses, and as time and science progressed, it was considered career-ending,” concluded Dr. Brusie. “Currently, veterinary medical sciences are so advanced that we have had great success with condylar fracture patients returning to full work. Luckily, with today’s advanced rehabilitation services, time, and help from mother nature, many horses can come back from an injury like this.”
Palm Beach Equine Clinic (PBEC) is changing the prognosis for condylar fracture injuries among sport horses. Advances in imaging, surgical talent, and the facilities necessary to quickly diagnose, treat, repair, and rehabilitate horses with condylar fractures have recently improved immensely.
Most commonly seen in Thoroughbred racehorses and occasionally polo ponies, a condylar fracture was once considered a career-ending injury. Today, however, odds are in favor of a full recovery with horses regularly returning to competition in their respective disciplines.
What is a Condylar Fracture?

A condylar fracture is a repetitive strain injury that results in a fracture to the cannon bone above the fetlock due to large loads transmitted during high-speed exercise. 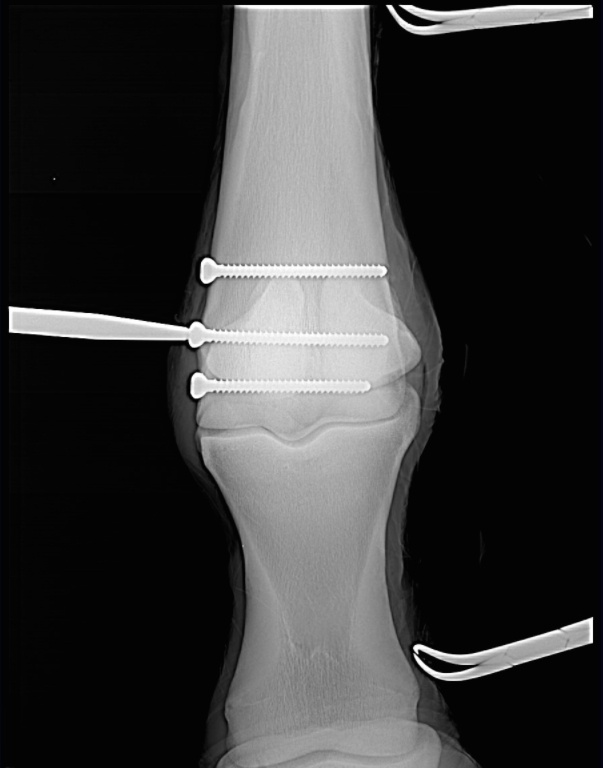
Scan showing the screws inserted during surgery (right). This patient, a Thoroughbred racehorse, walked away from surgery comfortably and is recovering well.
A condylar fracture is a repetitive strain injury that results in a fracture to the cannon bone above the fetlock due to large loads transmitted over the cannon bone during high-speed exercise. On a radiograph, a condylar fracture appears as a crack that goes laterally up the cannon from the fetlock joint and out the side of the bone, essentially breaking off a corner of the cannon bone, sometimes up to six inches long.
“A condylar fracture is a disease of speed,” said Dr. Robert Brusie, a surgeon at PBEC who estimates that he repairs between 30 and 50 condylar fractures per year. “A fracture to the left lateral forelimb is most common in racehorses as they turn around the track on a weakened bone and increased loading.”
Condylar fractures are further categorized into incomplete and non-displaced (the bone fragment hasn’t broken away from the cannon bone and is still in its original position), or complete and displaced (the fragment has moved away from the cannon bone itself and can often be visible under the skin).
Additionally, condylar fractures can occur laterally or medially. According to fellow PBEC surgeon Dr. Weston Davis, most condylar fractures tend to be lateral on the outside condyle (a rounded projection on a bone, usually for articulation with another bone similar to a knuckle or joint).
“Most lateral condylar fractures are fairly simple for us to fix,” said Dr. Davis. “Medial condylar fractures tend to be more complicated configurations because they often spiral up the leg. Those require more advanced imaging and more advanced techniques to fix.”
What is the Treatment?
The first step in effectively treating a condylar fracture through surgery is to accurately and quickly identify the problem. PBEC’s board-certified radiologist Dr. Sarah Puchalski utilizes the advanced imaging services at PBEC to accomplish exactly this.
“Stress remodeling can be detected early and easily on nuclear scintigraphy before the horse goes lame or develops a fracture,” said Dr. Puchalski. “Early diagnosis of stress remodeling allows the horse to be removed from active race training and then return to full function earlier. Early diagnosis of an actual fracture allows for repair while the fracture is small and hopefully non-displaced.”

Once the injury is identified as a condylar fracture, PBEC surgeons step in to repair the fracture and start the horse on the road to recovery. Depending on surgeon preference, condylar fracture repairs can be performed with the horse under general anesthesia, or while standing under local anesthesia. During either process, surgical leg screws are used to reconnect the fractured condyle with the cannon bone.
“For a very simple and small non-displaced fracture, we would just put in one to two screws across the fracture,” explains Dr. Davis. “The technical term is to do it in ‘lag fashion,’ such that we tighten the screws down heavily and really compress the fracture line. A lot of times the fracture line is no longer visible in x-rays after it is surgically compressed. When you get that good compression, the fractures heal very quickly and nicely.”
More complicated fractures, or fractures that are fully displaced, may require more screws to align the parts of the bone. For the most severe cases of condylar fractures, a locking compression plate with screws is used to stabilize and repair the bone.
PBEC surgeon Dr. Jorge Gomez, approaches a simpler non-displaced condylar fracture while the horse is standing, which helps to aid in a faster recovery and more successful surgical outcome.
“I will just sedate the horse and block above the site of the fracture,” said Dr. Gomez. “Amazingly, horses tolerate it really well. Our goal is always to have the best result for the horse, trainers, and us as veterinarians.”
According to Dr. Gomez, the recovery time required after a standing condylar fracture repair is only 90 days. This is made even easier thanks to a state-of-the-art surgery pit installed at PBEC. The four-and-a-half-foot recessed area allows doctors to perform surgeries on anything from a horse’s hock and below from a standing position. Horses can forgo the risks of general anesthesia for a mild sedative and local nerve blocks, greatly improving outcomes.

“A condylar fracture was once considered the death of racehorses, and as time and science progressed, it was considered career-ending,” concluded Dr. Brusie. “Currently, veterinary medical sciences are so advanced that we have had great success with condylar fracture patients returning to full work. Luckily, with today’s advanced rehabilitation services, time, and help from mother nature, many horses can come back from an injury like this.”
Fear of colic is in the back of many horse owners’ minds, but with the expert care of Palm Beach Equine Clinic, owners can rest easy knowing that they have some of the world’s best surgeons and veterinarians at their disposal in the event of an emergency.
Colic 101
Characterized by abdominal pain or problems with the gastrointestinal tract, colic is something that often arises unexpectedly and from many different origins. Spoiled feed, abrupt changes in feed, parasite infestation, sand ingestion, lack of water consumption, and even excess stress or changes in the weather are among the numerous causes generally related to colic.
Colic Symptoms
Whatever the cause may be, the most important step any owner can take is to recognize the symptoms as early as possible and immediately call their veterinarian. Pawing, rolling, looking at abdomen, sweating, loss of interest in food and water, and absence of gut sounds in any of the four abdominal quadrants are some of the telltale signs of colic development. Unfortunately, colic can be fatal, but the proper knowledge and care may save your horse’s life. The sooner your veterinarian gets involved in treatment, the better your horse’s chance of survival.

Emergency Colic Care
In the event of an emergency, the veterinarians and surgeons of Palm Beach Equine Clinic are available 24/7 to offer the very best care for your equine partner. Palm Beach Equine Clinic is renowned for its referral full-service surgical center and intensive care hospital located in the heart of Wellington, Florida. Board-Certified surgeons, primary care veterinarians, and skilled hospital technicians are available to treat, monitor, and care for critical cases. With world-class veterinarians and a full staff of highly trained technicians, both clients and patients of Palm Beach Equine Clinic are in the best hands possible.
Surgical Capabilities
Palm Beach Equine Clinic offers the latest in technology as the surgical techniques are less invasive and result in faster recovery times for your horse. The surgical team leader, Dr. Robert Brusie, is a nationally renowned, Board-Certified surgeon. Dr. Brusie’s surgical specialties include orthopedic, arthroscopic, and emergency cases. Dr. Brusie has been the head surgeon with PBEC for the past 20 years.
“In the last ten years, colic surgery has come a long, remarkable way,” Dr. Brusie stated. “With our clients, if the horse needs to go to surgery, we get an approximately 95% success rate. We attribute that to the client’s excellent care of their horses, as well as their knowledge to contact us immediately. That being said, colic surgery is always the last resort. We try to help all horses improve medically first.”
Palm Beach Equine’s surgical suite and staff is prepared to handle all types of emergencies, day and night. The large team of 40 veterinarians includes three Board-Certified Surgeons who rotate on-call duties so every day is covered. This aids Palm Beach Equine Clinic veterinarians and all of Southeast Florida with the ability to treat their emergencies requiring surgical assistance as quickly as possible. The state-of-the-art intensive care hospital is equipped with top-of-the-line medical equipment, including digital video cameras for the clinicians to easily monitor their patients from any location, at any time.

At Palm Beach Equine Clinic in Wellington, FL, the team of Board-Certified surgeons are experts in minimally invasive surgical techniques, aiming to reduce joint disease, resolve lameness, and improve the longevity of sport horse careers.

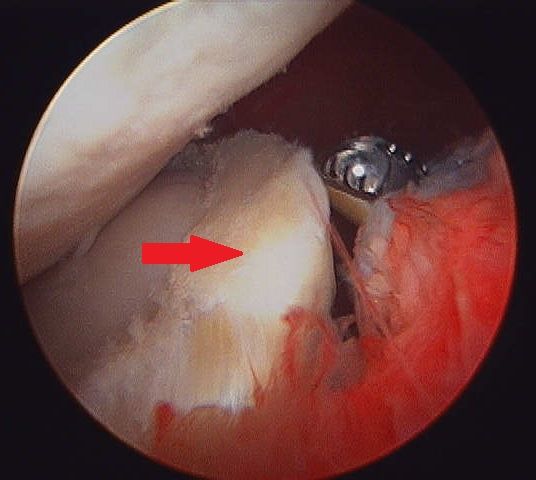
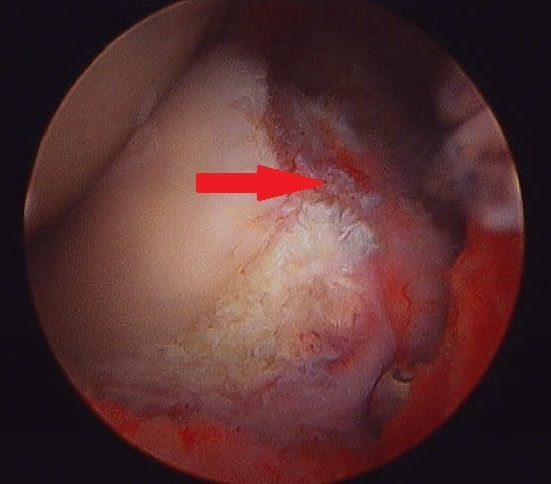
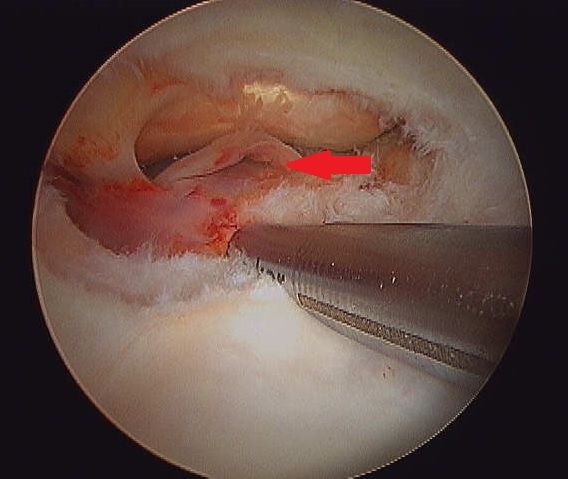
Arthroscopy (or arthroscopic surgery) is a minimally invasive surgical technique that can be performed on an injured joint or synovial structure to accurately explore and treat pathology. The surgery generally involves two very small (8mm) keyhole incisions. The first incision is where the surgeon will insert the arthroscope, which is an instrument with a small surgical grade camera installed that allows a complete, clear view of the interior joint surface. The second small incision is created to insert the surgical instrument to perform the procedure.
Arthroscopy is used to treat a broad range of injuries inside of a joint. Chip fracture removal is a procedure that is particularly commonly in both young Warmblood horses with developmental disease and in racehorses travelling at high speeds. A small chip fracture can cause persistent irritation in the joint as well as arthritis if left untreated. It is best removed immediately so that no further damage is created. The surgeon can go into the joint, remove the chip, and clean up the surrounding cartilage. Most horses recovery quickly and return to their normal athletic activity.
Board-Certified Surgeon Dr. Weston Davis performs many arthroscopic surgeries at Palm Beach Equine Clinic alongside fellow surgeons Dr. Robert Brusie and Dr. Jorge Gomez.
“In many horses, we consider arthroscopy as a prophylactic measure, intervening after injury, but before the development of a generalized degenerative arthritic cycle ensues,” Dr. Davis stated. “Arthroscopy is definitely something that you want to do early in the game if you feel like the horse has joint disease, or a chip, or cartilage disease, or an undefined injury that is not responding appropriately to medical therapy. Arthroscopy can be curative for some of these horses. But if you do not intervene early on in the course of the disease and there is already advanced arthritis, then you have missed your window.
“Arthroscopy is a preferred treatment because it is minimally invasive so most horses can go right back to work,” Dr. Davis continued. “In a typical scenario, we thoroughly explore the joint with the arthroscopic camera, we remove a chip or repair a lesion, and the horse is not lame after the surgery. Because of the small incisions, there is minimal aftercare and horses are often able to go back to work quickly.”
Other common indications for arthroscopic surgery are meniscal disease in the stifle, subchondral cystic lesions, primary cartilage lesions, and debridement of damaged tendinous/ligamentous tissue (such as deep digital flexor tendon tears in the navicular bursa). The surgeons at Palm Beach Equine Clinic can perform arthroscopy on virtually any joint in the horse. Anything from the Temporomandibular Joint (TMJ) of the head to the navicular bursa within the hoof capsule can be explored and treated with this minimally invasive approach.

Almost all arthroscopies are performed under general anesthesia with the horse on its back. New renovations at Palm Beach Equine Clinic include a set of stocks of adjustable height adjacent to a surgeon’s pit, allowing the surgeons to have eye-level access to the joint they are working on, enabling many new procedures on the legs of standing horses.
Minimally invasive surgery allows for a simple and quick recovery for the horse. The traditional horse would be on stall rest with a bandage on until the sutures come out at two weeks, and then start doing some light hand walking and physical therapy. Barring severe damage in the joint or associated tendon/ligament disruption, most cases will undergo a six-week rest and rehabilitation protocol, then return to normal work.
As always, the advanced diagnostic imaging at Palm Beach Equine Clinic permits the surgeons to get a complete evaluation of an injury involving a joint to ensure the best possible outcome. Depending on the injury type, digital radiographs, ultrasound, MRI, and Nuclear Scintigraphy, or a combination thereof, may be used for pre-operative diagnosis and planning. Ultrasound and digital radiography are available for intra-operative use. Intra-operative CT scanning will also be available in the future with the new additions at Palm Beach Equine Clinic.
“When you are inside the joint with an arthroscopic camera, you have the most complete picture of the surface and health of that joint,” Dr. Davis noted.
Palm Beach Equine Clinic (PBEC), located in Wellington, FL, offers advanced diagnostic imaging, world-renowned surgical talent, and state-of-the-art facilities necessary to quickly diagnose, treat, and repair horses with condylar fractures, making PBEC one of the leading facilities in the U.S. for condylar fracture repairs.
With thanks to the technology required for early diagnosis and experienced surgeons on staff, horses that are admitted to PBEC for condylar fracture repairs are more likely to return to training quickly. Most commonly seen in Thoroughbred racehorses and occasionally polo ponies or eventing horses, a condylar fracture was once considered a career-ending injury. Today, however, advances in technology aid in a full recovery with horses regularly returning to competition in their respective divisions.
What is a Condylar Fracture?
A condylar fracture is a repetitive strain injury that results in a fracture to the cannon bone above the fetlock due to large loads transmitted during high-speed exercise. On a radiograph, a condylar fracture appears as a crack that goes from the fetlock joint up the cannon bone. Lateral fractures many times exit the bone usually one-third of the way up the bone. Medial fractures will oftentimes spiral up to the hock or knee. Medial fractures are much more common in the hindlimb than the forelimb. It is the spiral fractures that are more difficult, due to the fact that the extent of the spiral cannot be identified radiographically. If the surgeon cannot identify the fracture, then that part of the fracture cannot be repaired.
“A condylar fracture is a disease of speed,” said Dr. Robert Brusie, a surgeon at PBEC who estimates that he repairs between 30 and 50 condylar fractures per year. “A fracture to the left lateral forelimb is most common in racehorses as they turn the track on a weakened bone and increased loading on the lateral condyle.”
Condylar fractures are further categorized into two classes. An incomplete and non-displaced fracture means that the bone fragment is not separated from the cannon and is still intact with its original position. A complete and displaced fracture means the fragment has detached from the cannon bone and this fracture can often be visible under the skin. Displaced condylar fractures have a somewhat lower prognosis due to the fact that soft tissue structures, such as the joint capsule, become torn. When these structures heal, they are thicker, which makes the joint less flexible.
“Most lateral condylar fractures are fairly simple for us to fix,” said PBEC surgeon Dr. Weston Davis. “Medial condylar fractures tend to be more complicated configurations because they often spiral up the leg. Those require more advanced imaging and more advanced techniques to fix.”
What is the Treatment?
The first step to effectively treating a condylar fracture through surgery is to accurately and quickly identify the problem. PBEC’s Board-Certified Radiologist Dr. Sarah Puchalski utilizes the advanced imaging services at PBEC to assist in the diagnosis.
“Stress remodeling can be detected early and easily on Nuclear Scintigraphy before the horse goes lame or even develops a fracture,” said Dr. Puchalski. “Early diagnosis of stress remodeling allows the horse to be removed from active race training and then return to full function earlier. Early diagnosis of an actual fracture allows for repair while the fracture is small and hopefully non-displaced.”
Once identified as a condylar fracture, PBEC surgeons step in to repair the fracture and start the horse on the road to recovery. Depending on surgeon preference, condylar fracture repairs can be performed with the horse under general anesthesia, or while standing under local anesthesia and sedation. During either process, surgical lag screws are used to reconnect the fractured condyle with the cannon bone.
“For a very simple and small non-displaced fracture, we would just put in one to two screws across the fracture,” explains Dr. Davis. “The technical term is to do it in ‘lag fashion’, such that we tighten the screws down heavily and compress the fracture line. Many times the fracture line is no longer visible in x-rays after it is surgically compressed. When you achieve good compression, the fractures heal very quickly and nicely.”
More complicated fractures, or fractures that are fully displaced, may require more screws to align parts of the bone. For the most severe cases of condylar fractures, a locking compression plate with screws is used to stabilize and repair the bone.
Severe condylar fractures often require general anesthesia, but for PBEC surgeon Dr. Jorge Gomez, approaching a simpler non-displaced condylar fracture while the horse is standing helps to aid in a faster recovery and successful surgical outcome.
“I think it takes the risk of anesthesia away and is a faster surgery from the time the horse comes in to the time the horse recovers,” said Dr. Gomez. “I will just sedate the horse and block above the site of the fracture. Amazingly, horses tolerate it really well, and it is very convenient for medial condylar fractures. In these cases, the fracture can spiral all the way up through the cannon bone, and they have a tendency to develop complete catastrophic fractures that can happen at any time after the injury. That risk can be significantly increased by the recovery from general anesthesia. Our goal is always to have the best result for the horse, trainers, and us, as veterinarians.”
According to Dr. Gomez, the recovery time required after a standing condylar fracture repair is only 90 days.
While Dr. Brusie, Dr. Davis, and Dr. Gomez are all seasoned in quickly and effectively repairing condylar fractures, PBEC is helping them to stay on the cutting edge of surgical techniques. PBEC is currently renovating its facility with plans to give surgeons a new approach to fix condylar fracture repairs. A set of stocks and surgeon’s pit have been added with the ability to give the surgeon eye-level access to the fracture with the patient standing and subsequently simplifying the procedure by reducing the risk from recumbent recovery.
What is the Prognosis?
One of the most common questions regarding an equine injury is, “Will the horse return to work?” Thanks to advanced imaging and surgical techniques, the answer to that question when involving a condylar fracture is most likely, “Yes.” At PBEC, a condylar fracture diagnosis rarely results in the end of a racehorse’s career.
Diagnostic imaging plays a major role in assisting to diagnose, surgically map, and follow up on condylar fractures. After primary use to diagnose a condylar fracture, digital radiographs are also used after surgery to ensure that a fracture repair was completely successful. According to Dr. Davis, scanning two planes during and after surgery gives a full view of the fracture and repair techniques, immediately indicating the success of the procedure before moving the horse on to recovery.
“A condylar fracture was once considered the death of racehorses, and as time and science progressed, it was considered career-ending,” said Dr. Brusie. “Currently, veterinary medical sciences are so advanced that we have had great success with condylar fracture patients returning to full work. Luckily, with today’s advanced rehabilitation services, time, and help from mother nature, many horses will come back from an injury like this.”
Palm Beach Equine Clinic provides experience, knowledge, availability, and the very best care for its clients. Make Palm Beach Equine Clinic a part of your team!